The
Resident
Personal Access
Acute Coronary Syndrome (ACS)
Labs
- BNP: <100 picograms per milliliter (pg/mL)
- BNP levels over 100 pg/mL may be a sign of heart failure
- Creatine kinase (CK): 20 to 200 U/L
Diagnostics
- Stress Test
- Exercise stress test
- Lexiscan (regadenoson) = pharmacological stress test
- Coronary Computed Tomography Angiography (CCTA)
- Helps to visualize calcification
- Right Heart Cath (RHC)
- Useful for pressure acquisition
- Left Heart Cath (LHC)
- Gold standard for coronary artery visualization
- Can perform PCI (stent placement) at the same time
- Instantaneous Wave-Free Ratio (iFR) – PCI treatment indicated if <0.89
- Fractional Flow Reserve (FFR) – PCI treatment indicated if <0.80
- Coronary Artery Assessment (via LHC)
- Right coronary artery (RCA)
- Left main coronary artery (LMCA):
- Left anterior descending (LAD) artery
- Left circumflex (LCx) artery
Notes
- DAPT Durations debatable – some literature suggests 3-6 months of DAPT, but 12 months remains the standard
- 1 month for bare metal stent
- 12 months for DES
- Can consider shorter duration for elective PCI (shorter duration DAPT trials inclusion criteria match this pt population)
- Switching between P2Y12 inhibitors
- If stent placed within 30 days: must load P2Y12 again
- If stent placed >30 days: do not have to load P2Y12
- If switching from clopidogrel or prasugrel: administer new drug at 24-hour mark
- If switching from ticagrelor: administer new drug at 12-hour mark
- Triple Antithrombotic Therapy (Afib/DVT/PE + ACS/PCI or CABG [DAPT optional, 30 days])
- ASA 81 + Clopidogrel (must be loaded, 300-600mg) + OAC
- Minimum 7 days if concomitant Afib/DVT/PE and ACS/PCI: 7-30 days
- After 30 days: drop aspirin (Expert Opinion d/t higher GI bleeding risk), continue P2Y12 Inhibitor + OAC
- Continue P2Y12 Inhibitor + OAC for 12 months
- After 12 months, drop P2Y12 and continue OAC indefinitely
- How to choose between 7-30 days of triple therapy*
- If one of the 4 main coronary arteries: 30 days
- If small vessels: 7-14 days (based on comorbidities, age, weight)
- *expert opinion/per institution
- ONLY clopidogrel can be used. If repeat STEMIs/NSTEMIs and failed clopidogrel, may use ticagrelor (benefit>risk)
- PPI: pantoprazole once daily for duration of triple therapy
- DAPT Extended Duration
- DAPT should be for 1 year minimum
- DAPT Score
- >2 = benefit to continue beyond 1 year
- <2 = no benefit of DAPT beyond 1 year
- Consider extended if recurrent ACS, rehospitalization for ACS, recurrence of stenting, etc.
- Post-MI LV Dysfunction
- Presents as HFrEF post-ischemic event
- Most often observed post-STEMI
- Not always necessary to treat with HFrEF GDMT
- SGLT2i no benefit in post-MI LV dysfunction
- Repeat Echo in 4 weeks to determine if reperfusion reversed LV dysfunction
- Presents as HFrEF post-ischemic event
Treatment
- Guideline recommended: initiation of beta blockers within 24 hours of ACS event is recommended (post-stent placement indication)
- Indicated for a duration of 3 years
- Debate due to REDUCE-AMI trial which showed no benefit of beta blockers
- NSTEMI Treatment Pillars
- Aspirin
- Statin
- Heparin (or Enoxaparin, treatment dose)
- LHC -> PCI: DAPT if catheterization occurs, BB if catheterization occurs
- Medication Management (no PCI/DES)
- Clopidogrel (only P2Y12 within indication), ASA 81, BB
- CABG
- Indications
- Triple vessel disease (RCA, LMCA: LAD, LCx)
- Left main (LCMA) blockage
- Discontinue ACE/ARBs 48 hours prior to surgery
- Discontinue Lovenox 1 dose prior to surgery
- Discontinue P2Y12i
- Plavix (Clopidogrel): 5 days prior
- Effient (Prasugrel): 7 days prior
- Brilinta (ticagrelor): 3-5 days prior
- Discontinue SGLT2i 48 hours prior for euvolemic DKA
- Post-procedural care:
- ASA monotherapy or:
- DAPT for 12 months
- Indications
- Angina + CCD
- 1st line: Antianginal therapy with either BB, CCB, or long-acting nitrate (Ex. Imdur [isosorbide mononitrate extended-release])
- If pt remains symptomatic, add second antianginal agent from different class
- 2nd line: Ranolazine
- Immediate relief: SL nitroglycerin, nitroglycerin spray
- Potentially harmful: ivabradine added to standard therapy
Medications
- Heparin
- CABG/PCI: continue heparin until revascularization
- Fibrinolytics: continue heparin for duration of hospital stay (maximum 8 days) or until revascularization
- Bivalirudin
- Useful in case of HIT reaction
- Fondaparinux
- Useful in case of HIT reaction
- P2Y12 Inhibitors
- Plavix (Clopidogrel)
- Loading dose: 300-600mg (administered in cath lab) (4hr vs 2hr onset of action, respectively)
- Maintenance dose: 75mg daily
- Irreversible platelet inhibitor (7-day life span of platelets)
- Weakest P2Y12 inhibitor
- Prodrug, 50% platelet inhibition
- *triple therapy eligible*
- Perioperative: Hold 5 DAYS before any surgery (do not give before stent has been deployed)
- Metabolism: CYP2C19 (1 in 4 patients are nonresponsive to clopidogrel due to genetic polymorphisms)
- ADE: risk of bleeding
- Effient (Prasugrel)
- Loading dose: 60mg
- Maintenance dose: 10mg daily
- Dose reduction: 5mg dose for <60kg, age >75
- Irreversible platelet inhibitor (7-day life span of platelets)
- Strongest P2Y12 inhibitor
- Prodrug, 70% inhibition
- Cannot use in medically managed pts (no studies)
- Perioperative: Hold 7 DAYS before any surgery (do not give before stent has been deployed)
- Warning/Caution: 5mg dose for <60kg, age >75
- Contraindication: STROKE or TIA (Black box)
- ADE: increased risk of bleeding
- Brilinta (ticagrelor)
- Loading dose: 180mg
- Maintenance dose: 90mg BID
- Reversible platelet inhibitor
- Non-prodrug, 70% inhibition
- Perioperative: Hold 3-5 DAYS before any surgery (do not give before stent has been deployed)
- Caution: COPD, interstitial lung disease
- Relative Contraindication: bradycardia (bradyarrythmia), any heart block
- Contraindication: CYP3A4 inhibitors, ASA >81mg
- Drug interactions: ASA >81mg, CYP3A4 inhibitors
- ADE: dyspnea
- Plavix (Clopidogrel)
- Nitrates
- Nitroglycerin
- Angina: 0.3 or 0.4 mg SL at onset. Repeat q5min x3 if angina persists (If pain is not relieved or worsens 3 to 5 minutes after 1 sublingual or translingual dose, seek immediate emergency medical attention)
- Refractory angina in ED: 0.6 mg single dose can be considered
- ADE: HA, hypotension
- Imdur (isosorbide mononitrate)
- Angina prevention, IR: 20 mg BID
- Angina prevention, ER: 30 to 60 mg once daily. Titrate up to 120 mg once daily. Max: 240 mg once daily.
- ADE: HA, hypotension, bradycardia, increased ICP
- Nitroglycerin
- Ranexa (Ranolazine)
- Angina, chronic stable: 500 mg twice daily. Max: 1,000 mg twice daily.
- ADE: QT prolongation
Anticoagulation
Virchow’s Triad
- Circulatory stasis
- Hypercoagulable state
- Endothelial injury
General VTE
- Maintenance Dose Treatment Duration
- Provoked: 3-6mo anticoagulation warranted
- Unprovoked: indefinite anticoagulation warranted
DVT
- Risk Stratification
- Wells’ Criteria
- Diagnostics
- D-Dimer (low specificity, high sensitivity), ultrasound, imaging studies, venography (gold standard)
- Treatment
- UHF
- PPX: 5000 units q8h SQ
- Treatment: 80 units/kg Bolus, 18 units/kg Infusion. Monitor and titrate according to protocol.
- LMWH
- PPX: 40mg daily SQ
- Treatment: 1mg/kg BID or 1.5mg/kg daily SQ
- Dose Adjustment: Renal
- UHF
PE
- Risk Stratification
- Wells’ Criteria
- Diagnostics
- D-Dimer, pulmonary angiography (gold standard), perfusion scans
- Treatment
- UHF
- PPX: 5000 units q8h SQ
- Treatment: 80 units/kg Bolus, 18 units/kg Infusion. Monitor and titrate according to protocol.
- LMWH
- PPX: 40mg daily SQ
- Treatment: 1mg/kg BID or 1.5mg/kg daily SQ
- Dose Adjustment: Renal
- UHF
Mechanical AVR (Warfarin)
- If risk factors present: goal INR = 2.5–3.5
- Requires bridge at therapeutic dose (heparin, enoxaparin, etc.)
- No risk factors present: goal INR = 2–3
- No bridge needed
- On-X valve (new)
- First 3 months: goal INR = 2–3
- >3 months: goal INR = 1.5–2
Transitioning Therapy
- Generally, dependent on half-life of agent
- Heparin → DOAC
- Give DOAC dose immediately (heparin low t1/2)
- DOAC → Heparin
- Start heparin at next dosing time (longer t1/2 for DOAC)
Medications
- Heparin
- DVT PPX: 5000 units q8h SQ
- DVT Treatment: 80 units/kg Bolus, 18 units/kg Infusion. Monitor and titrate according to protocol.
- Preferred over LMWH in ESRD, CKD5, AKI
- ADE: Thrombocytopenia/HIT (use direct thrombin inhibitors [urgent] or Xa inhibitor/warfarin [long term])
- Antidote: Protamine
- HIT: (Anecdotal) if platelets drop to <50, consider stopping heparin product. Switch to bivalirudin, argatroban, fondaparinux
- Enoxaparin (LMWH)
- DVT PPX: 40mg daily SQ
- BMI>40 = 40mg SQ BID
- <55kg or BMI<18: 30mg daily SQ
- DVT Treatment: 1mg/kg BID or 1.5mg/kg daily SQ
- Dose Adjustment: Renal (CrCl<30: 1mg/kg daily)
- ADE: Thrombocytopenia/HIT (use direct thrombin inhibitors [urgent] or Xa inhibitor/warfarin [long term])
- Antidote: Protamine
- HIT: (Anecdotal) if platelets drop to <50, consider stopping heparin product. Switch to bivalirudin, argatroban, fondaparinux
- DVT PPX: 40mg daily SQ
- Fondaparinux
- No HIT cross reactivity
- Q24h
- NO ANTIDOTE
- Direct Thrombin Inhibitors
- Argatroban, Bivalirudin, Lepirudin
- No HIT cross reactivity
- NO ANTIDOTE
- Warfarin (Vitamin K Inhibitor)
- 5mg/day initiation (lower for elderly, young)
- Interactions
- Higher effect: alcohol, CYP inhibitors, antibiotics, NSAIDs, Vitamin E
- Lower effect: CYP induction, binding (cholestyramine, sucralfate), VITAMIN K
- Monitor: PT or INR
- Antidote/Bleeding: Vitamin K (5-10mg slow IV), FFP, PCC (Kcentra), Recombinant VIIa
- Supratherapeutic INR
- INR >10 = Hold warfarin, Vitamin K1 2.5—5mg PO
- INR ≥4.5—10 = Omit 1—2 doses, Consider Vitamin K1 ≤5mg PO (2.5mg PO once or 5mg PO once)
- INR <4.5 = omit or lower dose
- Dosing Guide
- How Supplied: 1 mg, 2 mg, 2.5 mg, 3 mg, 4 mg, 5 mg, 6 mg, 7.5 mg, 10 mg
-
Example Warfarin Initiation Nomogram Targeting an INR Range of 2 to 3
Standard dosing for patients who are not expected to be sensitive to warfarin Reduced dosing for patients expected to be more sensitive to warfarin Initial dose 5 mg daily for 3 days 2.5 mg daily for 3 days Check INR the morning of day 4 <1.5 7.5 to 10 mg daily for 2 to 3 days 5 to 7.5 mg daily for 2 to 3 days 1.5 to 1.9 5 mg daily for 2 to 3 days 2.5 mg daily for 2 to 3 days 2 to 3 2.5 mg daily for 2 to 3 days 1.25 mg daily for 2 to 3 days 3.1 to 4 1.25 mg daily for 2 to 3 days 0.5 mg daily for 2 to 3 days >4 Hold until INR <3 -
Example Warfarin Maintenance Dosing Nomogram
Regular-intensity anticoagulation: INR goal 2 to 3 High-intensity anticoagulation: INR goal 2.5 to 3.5 Suggested adjustment(s) to warfarin dose Adjustment(s) for subtherapeutic (low) INR <1.5 <2 • Increase weekly maintenance dose by 10% to 20%
• Consider a one-time supplemental dose of 1.5 to 2 times the daily maintenance dose1.5 to 1.7 2 to 2.2 • Increase weekly maintenance dose by 5% to 15%
• Consider a one-time supplemental dose of 1.5 to 2 times the daily maintenance dose1.8 to 1.9 2.3 to 2.4 • No dosage adjustment may be necessary if the last 2 INRs were in range, if there is no clear explanation for the INR to be out of range, and, if in the judgment of the clinician, the INR does not represent an increased risk of thromboembolism for the patient; additional monitoring may be warranted
• If dosage adjustment needed, increase weekly maintenance dose by 5% to 10%
• Consider a one-time supplemental dose of 1.5 to 2 times the daily maintenance doseINR within therapeutic range 2 to 3 2.5 to 3.5 Desired range; no adjustment needed Adjustment(s) for supratherapeutic (high) INR 3.1 to 3.2 3.6 to 3.7 • No dosage adjustment may be necessary if the last 2 INRs were in range, if there is no clear explanation for the INR to be out of range, and, if in the judgment of the clinician, the INR does not represent an increased risk of hemorrhage to patient; additional monitoring may be warranted
• If dosage adjustment needed, decrease weekly maintenance dose by 5% to 10%3.3 to 3.4 3.8 to 3.9 • Decrease weekly maintenance dose by 5% to 10% 3.5 to 3.9 4 to 4.4 • Consider holding 1 dose
• Decrease weekly maintenance dose by 5% to 15%≥4 but ≤10 and no bleeding ≥4.5 but ≤10 and no bleeding • Hold until INR below upper limit of therapeutic range
• Decrease weekly maintenance dose by 5% to 20%
• If patient considered to be at significant risk for bleeding, consider low-dose oral vitamin K>10 and no bleeding >10 and no bleeding • Hold until INR below upper limit of therapeutic range
• Administer vitamin K orally
• Decrease weekly maintenance dose by 5% to 20% -
Warfarin: Adult Target INR Ranges Based Upon Indication
Indication Targeted INR Range Treatment Duration Cardiac Atrial fibrillation or atrial flutter 2 to 3 Indefinite LV thrombus, treatment 2 to 3 ~3 months after MI LV thrombus, prophylaxis for high-risk patients post MI 2 to 3 1 to 3 months after MI Acute Venous Thromboembolism Treatment Venous thromboembolism, provoked with a transient risk factor 2 to 3 3 months with reassessment for resolution of the provoking factor Venous thromboembolism, unprovoked or provoked with a persistent risk factor 2 to 3 ≥3 months depending on risk of VTE recurrence and bleeding Valvular (see “Valvular Heart Disease”)
-
Transition Guide
- Apixaban to warfarin: overlap apixaban with warfarin for ≥2 days until INR is therapeutic
- Rivaroxaban to warfarin: overlap rivaroxaban with warfarin for ≥2 days until INR is therapeutic
- Parenteral anticoagulant to warfarin: start warfarin and continue parenteral anticoagulant until INR is within therapeutic range (overlap parenteral anticoagulant with warfarin until INR is ≥2 for at least 2 days; duration of overlap is ~5 days)
- Warfarin to apixaban: discontinue warfarin and initiate apixaban as soon as INR falls to <2
- Warfarin to rivaroxaban: discontinue warfarin and initiate rivaroxaban as soon as INR falls to <3
- Warfarin to parenteral anticoagulation: stop warfarin and start the parenteral anticoagulant when INR is as close as possible to the lower end of the targeted INR range
- Miscellaneous
- Pregnancy: Category X
- Must overlap/bridge with Heparin/LMWH for active clot (4-5d) at therapeutic dose
- Genomics: VCORC1
- Protein binding high
- CYP metabolism
- Higher INR goal (3) for certain mechanical valves
- Warfarin-only indications: Tissue valve (surgical vs TAVR), Valvular heart disease, Mechanical valve*—aortic position, Mechanical valve—aortic position; afib or ↑ risk, Mechanical valves— mitral position, anti-phospholipid antibody syndrome
- Direct Oral Anticoagulants (DOACs)
- Life threatening bleed: 4-factor PCC, Andexanet alfa
- Pregnancy: do not use
- NOT IN:
- Valvular atrial fibrillation
- Mechanical valves
- Antiphospholipid antibody syndrome
- Rivaroxaban (Xarelto) (Xa Inhibitor)
- DVT Treatment: 15mg BID X3 weeks, then 20mg QD
- Afib: 20mg QD (15mg QD 30-50 CrCl)
- Post-op PPX: 10mg QD
- PAD (post revascularization): 2.5mg BID
- Administer with largest meal (usually dinner)
- Dose Adjustment: Renal
- Antidote: andexanet alfa
- Apixaban (Eliquis) (Xa Inhibitor)
- DVT Treatment: 10mg BID X7 days, then 5mg BID
- Afib: 5mg BID (2.5mg BID if any 2: Scr ≥ 1.5mg/dL, Age ≥80, Weight ≤60kg)
- Post-op PPX: 2.5mg BID
- Antidote: andexanet alfa
- Edoxaban (Savaysa) (Xa Inhibitor)
- DVT Treatment: 60mg QD AFTER 5-10 days parenteral tx (≤60kg or P-gp inhibitor or >50 CrCl = 30mg)
- Dose Adjustment: Renal (>95 or <50)
- Antidote: andexanet alfa
- Dabigatran (Praxada) (Direct Thrombin Inhibitor)
- DVT/PE Treatment: 150mg BID (AFTER parenteral anticoagulant)
- Afib: 150mg BID (>30 CrCl = 75mg BID)
- Antidote: Idarucizumab (Praxibind®), PCC
- IV Direct Thrombin Inhibitors
- Argatroban: weight based (0.5—2mcg/kg/min)
- Bivalirudin
Arrhythmias
- Presentation
- AF: P-Waves absent or irregular
- Paroxysmal AF: reverts back to normal rhythm spontaneously
- Attempt to convert to NSR
- Permanent AF: apparent each check (6+mo)
- Low chance of converting to NSR
- Aflutter
- Much better results with ablation
- Often times HR stuck at 150
- P waves at normal intervals, conduction ratios (2:1, 3:1, etc)
- RVR = >120BPM
- Rate controlled = <90BPM
- Risk Stratification
- CHA2DS2-VASc (Stroke Risk)
- ≥2 Men = OAC*
- ≥3 Women = OAC*
- *≥2 = OAC in most cases
- HAS-BLED (Bleed Risk)
- ≥3 = high bleed risk, use anticoagulant with caution
- CHA2DS2-VASc (Stroke Risk)
- Notes
- (Anecdotal) QT prolongation risk: prefer higher resting BPM to prevent arrythmia recurrence
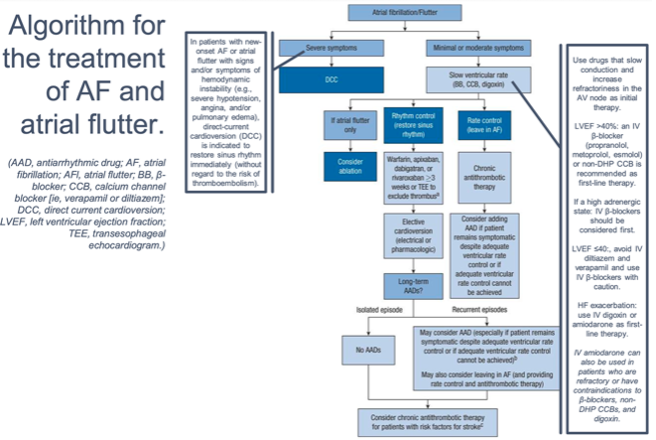
- Management
- AFFIRM trial (2002) – no significant difference between rate and rhythm groups
- Slightly higher mortality in rhythm group
- Guidelines
- 2019 AHA/ACC/HRS
- 2018 CHEST guidelines (antithrombotic therapy)
- Diagnostics
- Zio Patch / Holter Patch – worn on chest for 3-14 days. PVC >15% burden = first line: BB for rate control; second line: ablation
- Rate
- BB or non-DHP calcium channel blocker (diltiazem or verapamil)
- If hemodynamically unstable, cardioversion warranted
- Metoprolol tartrate: 2.5-5mg IV bolus (up to 3x), 12.5-100mg BID PO (Anecdotal: for acute phase arrythmias inpatient, consider q6h dosing)
- Metoprolol succinate: 50-400mg daily PO (Anecdotal: can use BID dosing for around-the-clock coverage)
- Propranolol: 1mg IV bolus (up to 3x), 10-40mg TID or QID
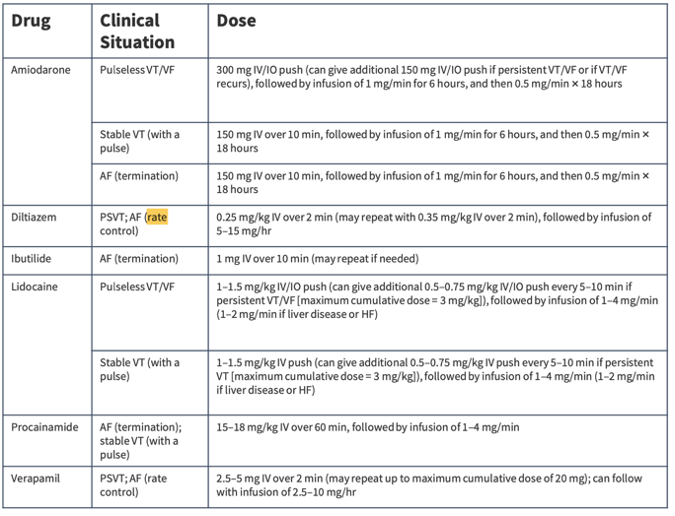
- Verapamil: 0.075-0.15 mg/kg IV bolus then 0.005 mg/kg/min infusion, 180-480 mg daily PO (ER)
- Diltiazem: 0.25 mg/kg IV bolus then 5-15 mg/h, 120-360 mg daily PO (ER)
- Amiodarone: 300 mg IV over 1h, then 10-50 mg/h over 24h, 100-200 mg daily PO
- Use caution initiating in younger individuals (ADEs with long term therapy)
- Can be used in HF
- 1g IV = 2g PO
- Digoxin: minimal hemodynamic effect (good for low SBP/MAPs, consider if BP makes metoprolol, etc. intolerable)
- Rhythm
- Cardioversion: AF/Flutter w/ RVR (unresponsive to pharmacological therapy), pre-excitation, or hemodynamic instability – Preferred to pharmacologic
- Ablation – preferred to pharmacologic
- Pharmacologic: Class III (ibutilide, dofetilide), Class Ic (flecainide, propafenone), and amiodarone (oral or IV) (Class IIb evidence for amiodarone)
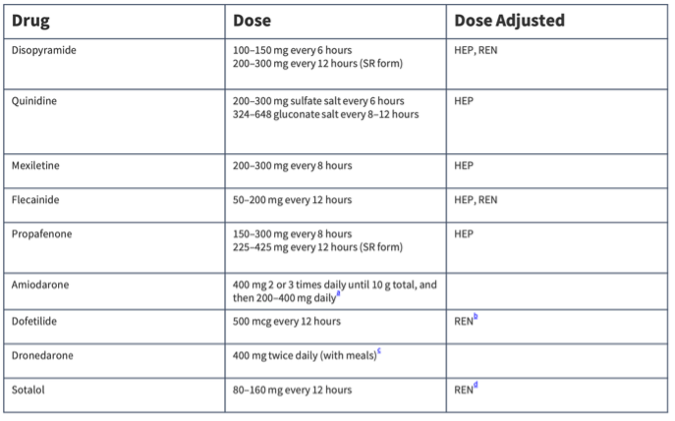
- Dofetilide: Conversion: 500mcg BID (Dose adjustment: renal). Can be used in HF. Maintain potassium >4 and magnesium in the normal range prior to initiation and during therapy.
- Flecainide: Conversion: >70 kg: 300 mg; <70 kg: 200 mg PO
- Propafenone: Conversion: >70 kg: 600 mg; <70 kg: 450 mg
- Consider atrioventricular (AV) nodal-blocking agent (eg, beta-blocker, nondihydropyridine calcium channel blocker) prior to initiation of Class Ic Antiarrhythmics (proarrhythmic effects -> rapid ventricular rate and hemodynamic compromise)
- Ibutilide: Conversion: 1mg over 10 min, repeat x1 if necessary
- Amiodarone (Class IIb evidence): Conversion: (PO) 600-800mg daily divided into doses until 10g load, then 200mg daily. (IV) 150mg over 10 min, then 1mg/min x6hr, then 0.5mg/min for 18hr
- Use caution initiating in younger individuals (ADEs with long term therapy)
- Can be used in HF
- 1g IV = 2g PO
- Ascension Conversion Policy: 150mg IV x1 -> 1mg/min x 6 hours -> 0.5mg/min x 18 hours -> THEN continue PO load @ 400mg BID x Xdays (AFib load = 5g total* Ventricular load = 10g total*) (*per institution)
- Calculate loading: includes IV (x2) + PO (x1) sources
- Maintenance doses = Afib 200mg daily, Ventricular 400mg daily
- typically 30-day duration post-cardioversion (electrical)
- AVOID flecainide and propafenone in SHD. Amio preferred.
- Pacemaker Placement
- Provides rate control
- Will not allow HR to drop below set point (Ex. continued metoprolol depressing HR)
- Can continue amiodarone/rhythm control agent post-placement for rhythm control
- Anticoagulation still recommended due to altered rhythm
- Concomitant Heart Failure
- HF rate control agents: GDMT beta blockers. If cannot tolerate, Digoxin Benefit: minimal hemodynamic effect (good for low SBP/MAPs, consider if BP makes metoprolol, etc. intolerable)
- HFrEF rhythm control agents: amiodarone or dofetilide
- HFpEF rhythm control agents: amiodarone, dronedarone, or dofetilide
- Anticoagulation (see CHA2DS2-VASc)
- Warfarin or DOAC: Prior to cardioversion (AF>48hr) for 3 weeks prior to cardioversion/ablation and 4 weeks after OR (AF < 48hr) immediately before and 4 weeks after OR high stroke risk (CHA2DS2-VASc)
- Anecdotal: EITHER anticoagulated 3 weeks prior and 4 weeks after cardioversion/ablation OR use TEE to check if clot in left atrial appendage (if no clot, proceed without anticoagulation, if not need anticoagulation prior)
- Always need 4 weeks anticoagulation post-cardioversion/ablation
- AFFIRM trial (2002) – no significant difference between rate and rhythm groups
- AF Algorithm
-
- Antiarrhythmic Maintenance Doses (PO)
-
- IV Antiarrhythmic Doses
-
Medications
- Rivaroxaban (Xarelto) (Xa Inhibitor)
- Afib: 20mg QD (15mg QD 30-50 CrCl)
- Administer with largest meal (usually dinner)
- Dose Adjustment: Renal
- Antidote: andexanet alfa
- Apixaban (Eliquis) (Xa Inhibitor)
- Afib: 5mg BID (2.5mg BID if any 2: Scr ≥ 1.5mg/dL, Age ≥80, Weight ≤60kg)
- Antidote: andexanet alfa
- Edoxaban (Savaysa) (Xa Inhibitor)
- 60mg QD AFTER 5-10 days parenteral tx (≤60kg or P-gp inhibitor or >50 CrCl = 30mg)
- Dose Adjustment: Renal (>95 or <50)
- Antidote: andexanet alfa
- Dabigatran (Praxada) (Direct Thrombin Inhibitor)
- Afib: 150mg BID (>30 CrCl = 75mg BID)
- Antidote: Idarucizumab (Praxibind®), PCC
Pericarditis
Treatment
- First Line
- ASA: 650–1000 mg q8h for ~6 months (no concern for uric acid increase)*
-
Ibuprofen: 600 mg q8h for ~6 months*
- *must prescribe PPI
- Second Line
- Colchicine: 0.6 mg BID for ~6 months
- Third Line
- Arcalyst (rilonacept): outpatient referral for registration and insurance adjudication
- Symptom Management – Steroids
- DO NOT USE for viral or idiopathic etiologies
-
Prednisone 0.2–0.5 mg/kg/day (Ex. 100 kg pt = 50 mg/day)
- Treatment dose for 2–4 weeks
- Taper by increments of ~5 mg over 2–3 months (long taper to prevent recurrence)
- Consider PJP PPX due to prolonged, high dose steroids (1 DS tablet daily)
Stroke/TIA
Assessment
- National Institutes of Health Stroke Scale (NIHSS): standardized assessment tool used to evaluate severity of stroke in patients
- 0 to 42, higher scores indicate greater neurological impairment
Thrombolytics
- Determine time from last well known
- Eligible for thrombolytics if <4.5h from onset
- Absolute Contraindications
- Prior intracranial hemorrhage
- Known structural cerebral vascular lesion
- Known malignant intracranial neoplasm
- Ischemic stroke within 3 months (excluding stroke within 3 hours*)
- Suspected aortic dissection
- Active bleeding or bleeding diathesis (excluding menses)
- Significant closed-head trauma or facial trauma within 3 months
- Relative Contraindications
- History of chronic, severe, poorly controlled hypertension
- Severe uncontrolled hypertension on presentation (SBP >180 mmHg or DBP >110 mmHg)
- History of ischemic stroke >3 months prior
- Traumatic or prolonged (>10 minutes) CPR or major surgery <3 weeks
- Recent (within 2 to 4 weeks) internal bleeding
- Noncompressible vascular punctures
- Recent invasive procedure
- For streptokinase/anistreplase – Prior exposure (>5 days ago) or prior allergic reaction to these agents
- Pregnancy
- Active peptic ulcer
- Pericarditis or pericardial fluid
- Current use of anticoagulant (eg, warfarin sodium) that has produced an elevated INR >1.7 or PT >15 seconds
- Age >75 years
- Diabetic retinopathy
Blood Pressure Control
- Maintain BP <185/110 before administration of thrombolytics (AHA)
Medications
- Alteplase
- Stroke: 0.9mg/kg (max dose = 90mg)
- 10% as IV bolus over 1 minute
- Remainder IV infusion over 60 minutes
- Stroke: 0.9mg/kg (max dose = 90mg)
- Tenecteplase
- Stroke
- 25mg/kg (max dose = 25mg) straight bolus
- <60kg = 15mg (3.0 mL)
- 60 to <70kg = 17.5mg (3.5 mL)
- 70 to <80kg = 20mg (4.0 mL)
- 80 to <90kg = 22.5mg (4.5 mL)
- ≥90kg = 25mg (5.0 mL)
- Stroke
Post-Thrombolytic Care
- Maintain BP <180/105
- Initiate high intensity statin
- ASA 81 + Clopidogrel x21d (DAPT x21d)
- Continue ASA 81 indefinitely
Valvular Heart Disease (VHD)
Notes
- MS associated with the highest risk of stroke
- Symptoms typically present only when severe disease exists
- TAVI
- Self-expanding = higher rates of heart block
- Surgically expanded = higher rate of rare complications
Valve Options
- Mechanical
- Often offered to younger individuals due to half-life of valve (20–30 years)
- Associated with higher thromboembolism = lifelong anticoagulation warranted
- Bioprosthetic
- Half-life of valve (10–15 years)
Aortic Stenosis (AS)
- Treatment
- SAVR
- <50 years old = typically mechanical
- TAVI
- SAVR
Aortic Regurgitation (AR)
- Treatment
- Valve repair/replacement is gold standard
- Medication Management (repair/replacement contraindicated)
- Vasodilators: decrease regurgitant flow, reduce SVP
Mitral Stenosis (MS)
- Highest risk of VTE/Stroke if left untreated
- Treatment
- Valve repair/replacement is gold standard
- Percutaneous mitral balloon commissurotomy (PMBC)
- Cannot be used if regurgitation present
- Rate control: BB or Non-DHP CCB
- Gentle diuresis: patients often present with heart failure-like volume overload
Mitral Regurgitation (MR)
- Treatment
- Primary MR: Valve repair/replacement is gold standard
- Secondary MR: HFrEF GDMT
- Mitral Clip
- DAPT for 3 months, then ASA monotherapy
Anticoagulation
-
Antithrombotic Therapy After Valve Replacement
Valve Drug Duration of Therapy Mechanical AVR, No Risk Factors Warfarin, INR goal = 2.0–3.0 Indefinite Mechanical On-X AVR, No Risk Factors 1. Warfarin, INR goal = 2.0–3.0
2. Warfarin, INR goal = 1.5–2.0 + Aspirin 75–100 mg1. First 3 months
2. ≥3 months after surgeryMechanical AVR with Risk Factors Warfarin, INR goal = 2.5–3.5 Indefinite Mechanical Mitral Valve Warfarin, INR goal = 2.5–3.5 Indefinite Bioprosthetic AVR 1. Warfarin, INR goal = 2.0–3.0
2. Aspirin 75–100 mg daily1. First 3–6 months
2. IndefiniteBioprosthetic MVR 1. Warfarin, INR goal = 2.0–3.0
2. Aspirin 75–100 mg daily1. First 3–6 months
2. IndefiniteTAVI Aspirin 75–100 mg daily Indefinite -
Antithrombotic Therapy in AF + VHD
AF Status Valve Drug Existing AF Rheumatic MS Warfarin, INR goal = 2.5 Native Valve Disease DOAC or VKA (CHA2DS2-VASc) Bioprosthetic Valve DOAC or VKA (CHA2DS2-VASc) New-Onset AF > 3 mo After Procedure Bioprosthetic Valve DOAC or VKA (CHA2DS2-VASc) New-Onset AF Within 3 mo After Procedure Bioprosthetic Valve Warfarin, INR goal = 2.5 N/A Mechanical Warfarin
Hypertension & Heart Failure PO Dosing Table
| Drug | Hypertension Initial | Hypertension Max | Heart Failure Initial | Heart Failure Max | Frequency | How Supplied |
|---|---|---|---|---|---|---|
| ARB | ||||||
| Candesartan | 16 mg | 32 mg | 4 to 8 mg | 32 mg | Daily | 4, 8, 16, 32 mg tablets |
| Irbesartan | 150 mg | 300 mg | – | – | Daily | 75, 150, 300 mg tablets |
| Losartan | 50 mg | 100 mg | 25–50 mg | 50–150 mg | Daily | 25, 50, 100 mg tablets |
| Olmesartan | 20 mg | 40 mg | – | – | Daily | 5, 20, 40 mg tablets |
| Telmisartan | 40 mg | 80 mg | – | – | Daily | 20, 40, 80 mg tablets |
| Valsartan | 80–160 mg | 320 mg | 20–40 mg BID | 160 mg BID | HTN Daily, HF BID* | 40, 80, 160, 320 mg tablets |
| ACEi | ||||||
| Benazepril | 10 mg | 40 mg | – | – | Daily | 5, 10, 20, 40 mg |
| Enalapril | 5–10 mg | 40 mg | 2.5 mg BID | 10–20 mg BID | Daily, BID | 2.5, 5, 10, 20 mg; OS, INJ |
| Captopril | 6.25–25 mg BID–TID | 50 mg TID | 6.25 mg TID | 50 mg TID | BID–TID | 12.5, 25, 50, 100 mg |
| Lisinopril | 5–10 mg | 40 mg | 2.5–5 mg | 20–40 mg | Daily | 2.5, 5, 10, 20, 30, 40 mg |
| Quinapril | 10–20 mg | 80 mg | 5 mg BID | 20 mg BID | Daily–BID | 5, 10, 20, 40 mg |
| Ramipril | 2.5 mg | 20 mg | 1.25–2.5 mg | 10 mg | Daily | 1.25, 2.5, 5, 10 mg |
| DHP CCB | ||||||
| Amlodipine | 2.5–5 mg | 10 mg | – | – | Daily | 2.5, 5, 10 mg |
| Nicardipine | 20 mg TID | 20–40 mg TID | – | – | TID | 20 mg, 30 mg |
| Nifedipine | 30 or 60 mg XL | 90 mg XL (120 mg XL reported) | – | – | Daily | IR: 10, 20 mg; XL: 30, 60, 90 mg |
| Non-DHP CCB | ||||||
| Diltiazem | 12hr: 60–120 mg BID 24hr: 120–240 mg Daily |
12hr: 240–360 mg in 2 doses 24hr: 120–360 mg Daily |
– | – | Daily–BID | 12hr: 60, 90, 120 mg 24hr: 120–420 mg |
| Verapamil | IR: 40–80 mg TID ER: 120 or 180 mg |
IR: 120–360 mg in 3 doses (max 480 mg/day) ER: 100–300 mg (max 400 mg) |
– | – | Daily–TID | IR: 40, 80, 120 mg ER: 120, 180, 240 mg |
| Thiazide Diuretics | ||||||
| Chlorthalidone | 12.5 to 25 mg | 25 mg | 12.5 to 25 mg | 100 mg | Daily | 25 mg, 50 mg |
| Hydrochlorothiazide | 12.5 to 25 mg | 50 mg | 25 mg daily or BID | 100 mg | Daily | 12.5 mg, 25 mg, 50 mg |
| Indapamide | 1.25 to 2.5 mg | 2.5 mg | – | – | Daily | 1.25 mg, 2.5 mg |
| Metolazone | – | – | 2.5-5 mg | 20 mg | Daily | 2.5 mg, 5 mg, 10 mg |
| Aldosterone Antagonists | ||||||
| Eplerenone | 50 mg | 50 mg BID | 25 mg | 50 mg | Daily-BID | 25 mg, 50 mg |
| Spironolactone | 12.5 to 25 mg | 50 to 100 mg | 12.5 to 25 mg | 50 mg | Daily | 25 mg, 50 mg, 100 mg |
| Alpha-1 Blockers | ||||||
| Doxazosin | 1 mg | 16 mg | – | – | Daily | 1 mg, 2 mg, 4 mg |
| Prazosin | 1 mg BID-TID | 20 mg/day in 2-3 doses | – | – | BID-TID | 1 mg, 2 mg, 5 mg |
| Terazosin | 1 mg | 20 mg/day in 1-2 doses | – | – | Daily-BID | 1 mg, 2 mg, 5 mg, 10 mg |
| Beta Blockers | ||||||
| Atenolol (cardioselective) | 25 mg daily or BID | 100 mg/day in 1-2 doses | – | – | Daily-BID | 25 mg, 50 mg, 100 mg |
| Bisoprolol (cardioselective) | 2.5 to 5 mg | 2.5 to 10 mg, Max: 20 mg | 1.25 mg | 10 mg | Daily | 2.5 mg, 5 mg, 10 mg |
| Metoprolol tartrate (cardioselective) | 50 mg BID | 100 to 200 mg/day in 2 doses, Max: 400 mg | – | – | BID* | 25 mg, 37.5 mg, 50 mg, 75 mg, 100 mg |
| Metoprolol succinate (cardioselective) | 25 to 100 mg | 50 to 200 mg, Max: 400 mg | 12.5 to 25 mg | 200 mg | Daily | 25 mg, 50 mg, 100 mg, 200 mg |
| Carvedilol (combined alpha + beta) | IR: 6.25 mg BID ER: 20 mg |
IR: 6.25 to 25 mg BID, Max: 50 mg/day ER: 20 to 80 mg |
IR: 3.125 mg BID ER: 10 mg |
IR: ≤85 kg: 25 mg BID >85 kg: 50 mg BID ER: 80 mg |
Daily-BID | IR: 3.125 mg, 6.25 mg, 12.5 mg, 25 mg ER: 10 mg, 20 mg, 40 mg, 80 mg |
| Labetalol (combined alpha + beta) | 100 mg BID | 200 to 800 mg/day in 2 doses | – | – | BID | 100 mg, 200 mg, 300 mg, 400 mg |
| Nebivolol (cardioselective and vasodilatory) | 5 mg | 40 mg | – | – | Daily | 2.5 mg, 5 mg, 10 mg, 20 mg |
| Nadolol (nonselective) | 40 mg | 40 to 120 mg, Max: 320 mg | – | – | Daily | 20 mg, 40 mg, 80 mg |
| Propranolol (nonselective) | 80 mg/day in 1-4 doses | 80 to 160 mg/day in 1-4 doses | – | – | Daily-BID-TID-QID | IR: 10 mg, 20 mg, 40 mg, 60 mg, 80 mg ER: 60 mg, 80 mg, 120 mg, 160 mg |
| Acebutolol (sympathomimetic) | 200 to 400 mg in 1-2 doses | 200 to 800 mg/day in 1-2 doses, Max: 1,200 mg/day | – | – | Daily-BID | 200 mg, 400 mg |
| Loop Diuretics | ||||||
| Furosemide | – | – | 20–40 mg daily or BID | 80 to 200 mg max single dose, Max: 600 mg/day | Daily-BID-TID | 20 mg, 40 mg, 80 mg |
| Torsemide | 5 mg | 10 mg | 10–20 mg daily or BID | 50 to 100 mg, Max: 200 mg in 2 doses | Daily-BID | 5 mg, 10 mg, 20 mg, 100 mg |
| Bumetanide | – | – | 0.5–1 mg daily or BID | 3 to 10 mg max single dose, Max: 10 mg/day | Daily-BID-TID | 0.5 mg, 1 mg, 2 mg |
| Potassium-Sparing Diuretics | ||||||
| Amiloride | 5 mg | 10 mg/day in 1-2 doses | – | – | Daily | 5 mg |
| Triamterene | – | – | 50 to 100 mg | 300 mg/day | Daily-BID | 50 mg, 100 mg |
| Alpha-2 Adrenergic Agonists | ||||||
| Clonidine | 0.1 mg BID, 0.1 mg/wk (patch) | 0.2 to 0.6 mg/day in 2-3 doses, Max: 2.4 mg 0.1 to 0.3 mg/wk (patch) |
– | – | BID-TID-qWK | Patch: 0.1, 0.2, 0.3 mg/24hr Tablet: 0.1 mg, 0.2 mg, 0.3 mg |
| Methyldopa | 250 mg BID-TID | 250 mg to 1 g in 2-4 doses, Max: 3 g/day | – | – | BID-TID-QID | 250 mg, 500 mg |
| Guanfacine | 0.5 to 1 mg | 2 mg | – | – | Daily | IR: 1 mg, 2 mg ER: 1 mg, 2 mg, 3 mg, 4 mg |
| Direct Renin Inhibitor | ||||||
| Aliskiren | 150 mg | 300 mg | – | – | Daily | 150 mg, 300 mg |
| Direct Vasodilators | ||||||
| Hydralazine | 10 mg QID | 100 to 200 mg/day in 4 doses, Max: 300 mg/day | 25 mg TID + iso. dinit. | 75 or 100 mg TID + iso. dinit. | TID-QID | 10 mg, 25 mg, 50 mg, 100 mg |
| Minoxidil | 5 mg | 10 to 40 mg/day in 1-3 doses, Max: 100 mg/day | – | – | Daily-BID-TID | 2.5 mg, 10 mg |
| ARNI | ||||||
| Entresto (sacubitril and valsartan) | – | – | 24 mg/26 mg or 49 mg/51 mg* BID | 97 mg/103 mg BID | BID | 24 mg/26 mg, 49 mg/51 mg, 97 mg/103 mg |
| SGLT2i | ||||||
| Farxiga (dapagliflozin) | – | – | 10 mg | 10 mg | Daily | 5 mg, 10 mg |
| Jardiance (empagliflozin) | – | – | 10 mg | 10 mg | Daily | 10 mg, 25 mg |
| Nitrates | ||||||
| Isosorbide dinitrate | – | – | 20 mg TID + hydral | 40 mg TID + hydral | TID | 5 mg, 10 mg, 20 mg, 30 mg, 40 mg |